
IVF Suitability Checker
IVF Suitability Assessment
This tool helps identify potential medical reasons why IVF might not be appropriate for you or your partner. Based on your responses, it will provide insights into whether IVF may be suitable or if you should consider other options.
Please answer the following questions:
IVF isn’t a magic solution for every couple struggling to conceive. While it’s helped millions of people become parents, it’s not safe-or even possible-for everyone. Some medical conditions make IVF unlikely to work, dangerously risky, or outright inappropriate. Knowing who should avoid IVF can save time, money, and emotional pain.
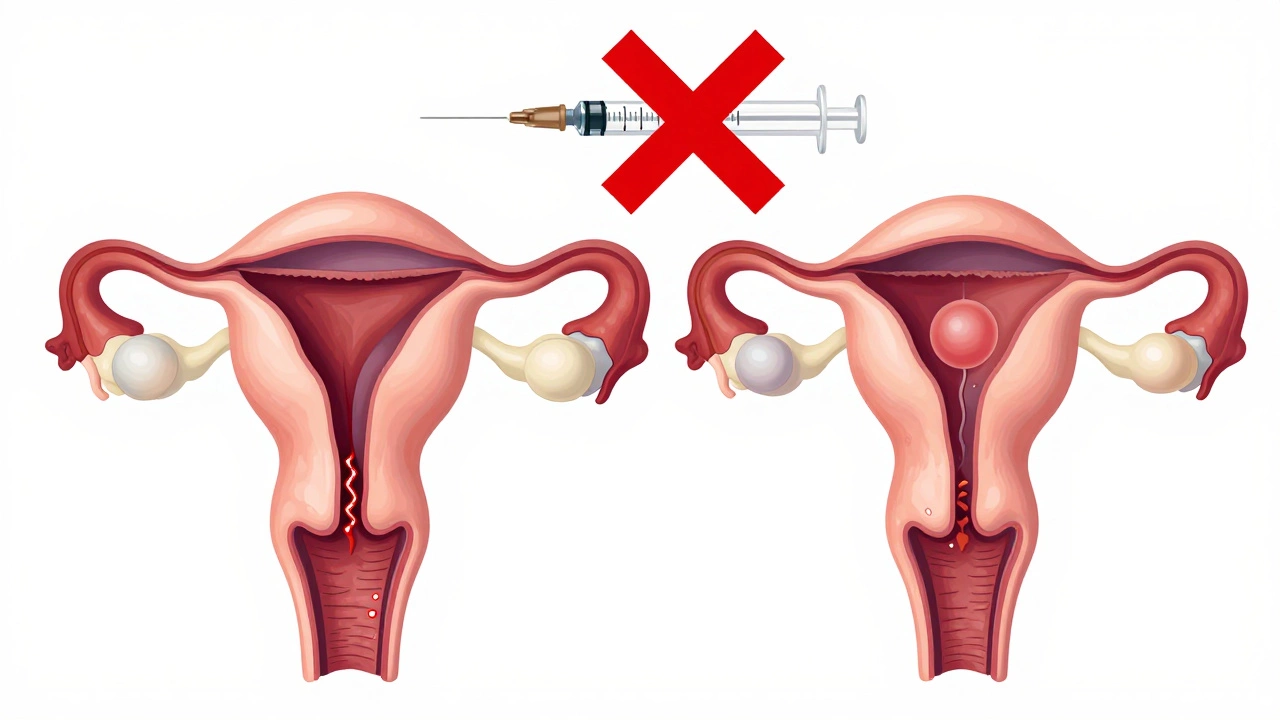
Women with severe uterine abnormalities
If the uterus is missing, severely scarred, or structurally damaged, IVF won’t help. The embryo needs a place to implant and grow. If the uterine lining is too thin, or if there are large fibroids blocking the cavity, pregnancy won’t stick-even if the embryo is perfect. Conditions like Mayer-Rokitansky-Küster-Hauser syndrome, where the uterus doesn’t develop, mean IVF is useless without a gestational carrier. Even in cases of severe Asherman’s syndrome (intrauterine adhesions), repeated surgeries may be needed before IVF has any chance. Without a functional uterus, IVF is just a costly cycle of hope.
Women with untreated serious medical conditions
Pregnancy puts major stress on the body. If you have uncontrolled diabetes, severe heart disease, or advanced kidney failure, IVF can be life-threatening. High blood pressure during pregnancy raises the risk of preeclampsia, stroke, and organ damage. For women with Class III or IV heart disease (according to the WHO classification), the strain of carrying a baby can lead to heart failure. Diabetes that isn’t tightly managed increases the chance of miscarriage, birth defects, and premature delivery. Before even starting IVF, doctors require these conditions to be stable-often for months. If they can’t be stabilized, IVF is off the table.
Women with active cancer or recent cancer treatment
IVF requires high doses of hormones that stimulate the ovaries. For women with hormone-sensitive cancers-like estrogen-receptor-positive breast cancer-this can fuel tumor growth. Even if the cancer is in remission, most oncologists recommend waiting at least two years before attempting pregnancy. The stress of IVF and pregnancy can interfere with follow-up scans, medications, and recovery. Some chemotherapy drugs permanently damage the ovaries, making egg retrieval impossible. In these cases, egg freezing before cancer treatment is the better path. Starting IVF during active cancer treatment is medically irresponsible.
Women over 45 with very low ovarian reserve
Age isn’t just a number in IVF. By 45, the chance of a woman’s own eggs resulting in a live birth is less than 1%. Most clinics won’t even attempt IVF with a woman’s own eggs after 44. The risk of miscarriage jumps to over 50%, and chromosomal abnormalities like Down syndrome become far more likely. Even if an embryo implants, the chance of carrying to term is low. Some clinics offer IVF with donor eggs for women up to 50, but using your own eggs past 45 is rarely successful and often leads to repeated emotional and financial loss. If you’re over 45 and still hoping for a biological child, donor eggs are the only realistic option.
Men with no sperm production (non-obstructive azoospermia)
IVF needs sperm. If a man has non-obstructive azoospermia-meaning his testicles don’t make sperm at all-then standard IVF won’t work. In some cases, a testicular biopsy might find a few sperm cells, but if none are found after multiple attempts, IVF isn’t possible. This happens in about 10-15% of severe male infertility cases. Without sperm, even ICSI (a technique where a single sperm is injected into an egg) can’t be done. Couples in this situation must consider donor sperm or adoption. Pushing forward with repeated IVF cycles without sperm is a waste of resources and hope.
Couples with untreated genetic disorders
If both partners carry the same serious genetic condition-like Tay-Sachs, cystic fibrosis, or spinal muscular atrophy-IVF without preimplantation genetic testing (PGT) could result in a child with a fatal disease. Even with PGT, some couples choose not to proceed because they don’t want to discard affected embryos. But if they refuse testing and still pursue IVF, they’re knowingly risking a child’s life. Clinics will often require genetic counseling and testing before starting IVF for couples with known hereditary conditions. Skipping this step isn’t just risky-it’s unethical.
People with untreated mental health conditions
IVF is emotionally grueling. The hormone injections, constant monitoring, failed cycles, and financial pressure can trigger or worsen depression, anxiety, or bipolar disorder. If someone is in the middle of an active psychotic episode, severe depression with suicidal thoughts, or uncontrolled PTSD, IVF can make things worse. Many clinics require psychological screening before starting treatment. If someone isn’t stable, therapists and doctors will often delay IVF until mental health is managed. It’s not about judging someone’s strength-it’s about protecting their well-being during a process that demands emotional resilience.
People who can’t afford the long-term costs
IVF isn’t a one-time expense. One cycle costs $12,000 to $20,000 in the U.S., and most people need 2-3 cycles to succeed. Add in medications ($3,000-$7,000 per cycle), genetic testing, storage fees, and potential complications like ovarian hyperstimulation syndrome (OHSS), and the total can hit $50,000. If a couple doesn’t have savings, insurance coverage, or a solid financial plan, they risk bankruptcy. Some end up in debt for years, even after a failed cycle. IVF clinics often require financial counseling before treatment. It’s not about money being a moral issue-it’s about avoiding a cycle of financial trauma on top of infertility grief.
People who don’t understand the risks
Some people think IVF is a guaranteed path to parenthood. It’s not. Success rates drop sharply with age. Multiple births are common, and twins or triplets come with higher risks of preterm birth, cerebral palsy, and developmental delays. Ovarian hyperstimulation syndrome can cause severe pain, fluid buildup, and even kidney failure. There’s also a small but real risk of ectopic pregnancy or ovarian torsion. If someone doesn’t fully understand these risks-or is being pressured by family or social expectations-they’re not ready for IVF. Informed consent isn’t a formality. It’s a requirement.
What happens if someone ignores these red flags?
When IVF is attempted despite clear medical warnings, the outcomes are often painful. A woman with uncontrolled diabetes might miscarry three times before realizing her body can’t sustain a pregnancy. A couple with untreated genetic risks might give birth to a child with a fatal condition, facing years of medical care and grief. A man with no sperm might drain his savings on repeated, futile cycles. The emotional toll is just as heavy as the physical one. Many people who ignore these warnings end up more broken than when they started.
Alternatives to IVF when it’s not an option
Even if IVF isn’t right for you, parenthood is still possible. Adoption, foster care, and donor sperm or eggs are real paths. Surrogacy works for women without a uterus. Some couples choose to live child-free and find fulfillment in other ways. There’s no shame in choosing a different path. The goal isn’t IVF-it’s building a family in a way that’s safe, sustainable, and emotionally healthy.
Can you get IVF if you have PCOS?
Yes, many women with PCOS successfully get pregnant with IVF. However, they’re at higher risk for ovarian hyperstimulation syndrome (OHSS). Doctors manage this by using lower doses of medication and monitoring closely. PCOS alone doesn’t disqualify someone from IVF-it just requires careful planning.
Is IVF possible after menopause?
With your own eggs? No. After menopause, the ovaries stop producing eggs. But IVF using donor eggs is still possible for women up to their early 50s. The uterus can still carry a pregnancy, even without natural hormone production. Hormone therapy prepares the lining for embryo transfer.
Can you get IVF if you’re overweight?
Being overweight doesn’t automatically disqualify you, but it lowers success rates and increases risks. Obesity raises the chance of miscarriage, gestational diabetes, and complications during egg retrieval. Many clinics recommend losing 5-10% of body weight before starting IVF to improve outcomes.
Does age matter more than health for IVF?
Age is the biggest factor in IVF success because egg quality declines sharply after 35. But health matters too. A healthy 42-year-old might have better odds than an unhealthy 32-year-old with severe endometriosis or diabetes. Both factors must be weighed together.
Can you get IVF if you’ve had cancer surgery?
It depends on the type of cancer, treatment, and time since recovery. For most cancers, doctors wait 1-2 years after treatment before allowing IVF. If the cancer was hormone-sensitive, they’ll check estrogen levels carefully. If you’re in remission and cleared by your oncologist, IVF with donor eggs or your own frozen eggs may be possible.
Final thoughts
IVF is powerful, but it’s not a cure-all. The most successful outcomes come from people who understand their limits-and respect them. Saying no to IVF isn’t failure. It’s wisdom. Choosing a safer, more realistic path to parenthood-or choosing a child-free life-can lead to deeper peace than forcing a process that could harm you. The goal isn’t to have a baby at all costs. It’s to build a life that’s healthy, whole, and sustainable.




Write a comment