
Diabetes Medication Matchmaker
Answer these questions to discover which diabetes medication class might align best with your health profile and goals.
Lower A1C Fast
Maximize blood sugar reduction
Lose Weight
Weight loss is a priority
Protect Organs
Heart & kidney protection
Yes
I have heart disease, heart failure, or chronic kidney disease
No
No known heart or kidney conditions
Prefer Pills
I'd rather take oral medications
Open to Injections
If it's more effective, I'm open to injectables
Yes, Cost Matters
I need affordable/generic options
Less Concerned
I have good insurance or can afford newer medications
Your Personalized Recommendation
Your A1C number is more than just a statistic on a lab report. It is the average of your blood sugar levels over the past two to three months. If that number is creeping up, you are likely looking for the most effective way to bring it down quickly and safely. But here is the hard truth: there is no single "best" medicine for everyone. The right choice depends entirely on your body, your budget, and other health conditions like heart disease or kidney function.
In 2026, we have moved far beyond just insulin and basic pills. We now have powerful classes of drugs that not only lower glucose but also protect your heart and help with weight loss. This guide breaks down the top contenders so you can have a smarter conversation with your doctor.
The Gold Standard: Metformin
If you have been diagnosed with type 2 diabetes, your doctor probably started you on Metformin, which is a biguanide medication that decreases glucose production in the liver and improves insulin sensitivity. It remains the first-line treatment for millions of people worldwide. Why? Because it works, it is cheap, and it has been studied for decades.
Metformin typically lowers A1C by about 1% to 1.5%. It does not cause hypoglycemia (low blood sugar) on its own, and it often leads to modest weight loss. However, it is not magic. Some people experience stomach upset, diarrhea, or nausea when they start. Taking it with food usually helps. If you have significant kidney issues, your doctor might avoid this drug because your kidneys need to clear it from your system.
The Heavy Hitters: GLP-1 Receptor Agonists
If lowering A1C was a race, GLP-1 receptor agonists are currently injectable medications that mimic the incretin hormone GLP-1 to stimulate insulin release, slow digestion, and reduce appetite. These drugs have taken the medical world by storm. They don't just lower blood sugar; they transform how patients feel about their health.
| Medication Name | Dosing Frequency | Average A1C Reduction | Key Benefit |
|---|---|---|---|
| Semaglutide (Ozempic/Wegovy) | Once weekly | 1.5% - 2.5% | Significant weight loss and cardiovascular protection |
| Tirzepatide (Mounjaro/Zepbound) | Once weekly | 2.0% - 3.0% | Highest A1C reduction; dual GIP/GLP-1 action |
| Dulaglutide (Trulicity) | Once weekly | 1.0% - 1.8% | Well-tolerated, proven heart benefits |
Tirzepatide is particularly notable because it targets two hormones (GIP and GLP-1), making it potentially more potent than older GLP-1s. Clinical trials show it can drop A1C by nearly 2.5% on average. The downside? They are injections, they can be expensive if insurance doesn't cover them, and side effects like nausea are common during the first few weeks as your dose increases.
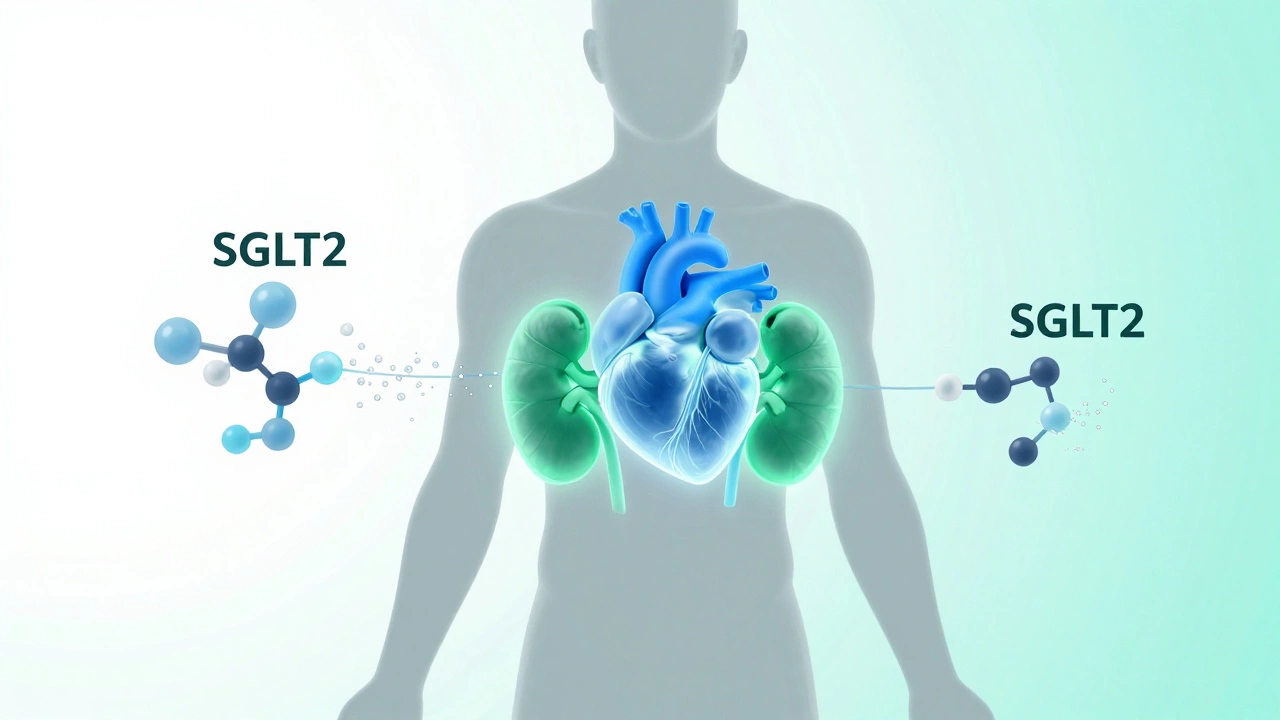
Heart and Kidney Protectors: SGLT2 Inhibitors
You might not think of your urine as a tool for lowering blood sugar, but SGLT2 inhibitors are oral medications that block the reabsorption of glucose in the kidneys, causing excess sugar to be excreted in urine. Drugs like Empagliflozin (Jardiance) and Dapagliflozin (Farxiga) work by flushing out sugar through your pee.
This mechanism is unique. While they lower A1C by about 0.5% to 1%, their real superpower is protecting your organs. Major studies have proven that SGLT2 inhibitors significantly reduce the risk of hospitalization for heart failure and slow the progression of chronic kidney disease. If you have heart or kidney issues alongside diabetes, these are often considered the "best" medicine for you, even if another drug lowers A1C slightly more.

Old School Reliability: Sulfonylureas
Sulfonylureas are older oral medications that stimulate the pancreas to produce more insulin regardless of blood sugar levels. Examples include glipizide and glimepiride. They are incredibly effective at lowering A1C, often dropping it by 1% to 2%. They are also very cheap.
However, they come with a catch. Because they force your pancreas to pump out insulin, they carry a higher risk of hypoglycemia (dangerously low blood sugar). They can also cause weight gain. Today, doctors usually reserve sulfonylureas for patients who cannot afford newer drugs or who do not respond to metformin alone. They are effective, but they require careful monitoring.
When Insulin Is Necessary
For some people, especially those with type 1 diabetes or advanced type 2 diabetes where the pancreas has burned out, oral meds and non-insulin injections aren't enough. Insulin therapy is the administration of the hormone insulin to regulate blood glucose levels, available in various forms including rapid-acting, long-acting, and premixed options. Insulin is the most powerful tool we have. It can lower A1C from 12% to 7% in a matter of weeks.
The challenge with insulin is management. You have to monitor your blood sugar frequently, adjust doses based on food and activity, and deal with the risk of lows. Modern pens and continuous glucose monitors (CGMs) have made this easier, but it is still a commitment. If your A1C is above 10% or you have symptoms like extreme thirst and fatigue, your doctor will likely start you on insulin immediately to get you safe.
How to Choose the Right Path
Choosing the best medicine isn't just about picking the one with the biggest A1C drop. It is about matching the drug to your life. Ask yourself these questions:
- Do I have heart or kidney disease? If yes, prioritize SGLT2 inhibitors or GLP-1s.
- Is weight loss a goal? GLP-1s and Tirzepatide are superior for weight management.
- Am I worried about cost? Metformin and Sulfonylureas are generic and affordable. Newer injectables can cost thousands without insurance coverage.
- Do I hate needles? Stick to oral meds like Metformin, SGLT2s, or DPP-4 inhibitors (like Sitagliptin).
Often, the "best" approach is combination therapy. Starting with Metformin and adding an SGLT2 inhibitor or a GLP-1 agonist allows you to hit your A1C target while protecting your heart and managing weight. This multi-drug approach is becoming the standard of care in 2026.
Lifestyle: The Silent Partner
No pill works well if you ignore lifestyle factors. Medication reduces the burden on your body, but diet and exercise do the heavy lifting. Cutting back on refined carbohydrates and added sugars has an immediate impact on post-meal spikes. Regular physical activity, even just walking 30 minutes a day, makes your cells more sensitive to insulin, allowing whatever medication you take to work better.
Can I lower my A1C without medication?
In early stages of prediabetes or mild type 2 diabetes, significant lifestyle changes-such as losing 5-10% of body weight, adopting a low-carb or Mediterranean diet, and exercising regularly-can sometimes lower A1C enough to delay or avoid medication. However, for many people, genetics play a strong role, and medication is necessary to reach safe levels.
Which medicine causes the least weight gain?
GLP-1 receptor agonists (like Semaglutide and Tirzepatide) and SGLT2 inhibitors are associated with weight loss. Metformin is generally weight-neutral or causes slight weight loss. In contrast, insulin, sulfonylureas, and thiazolidinediones often cause weight gain.
How quickly do these medicines work?
Most oral medications like Metformin show effects within days, but A1C reflects a 3-month average, so you won't see the full result in your blood test until then. Insulin works immediately to lower blood sugar. GLP-1s may take several weeks to reach their full potential as doses are gradually increased to minimize side effects.
Are GLP-1 injections covered by insurance?
Coverage varies widely by insurer and region. Many plans cover them for diabetes treatment but may restrict use for weight loss alone. Prior authorization is often required. Always check with your specific provider and ask about patient assistance programs offered by pharmaceutical companies.
What is the safest medicine for kidneys?
SGLT2 inhibitors are actually protective for kidneys, slowing disease progression. Metformin needs dose adjustments or cessation if kidney function drops below a certain threshold (eGFR <30-45). DPP-4 inhibitors like Linagliptin are also safe for all levels of kidney function without dose adjustment.



Write a comment